Raham Hasan Mostafa1,*, Ashraf Nabil Saleh1, Shaimaa M.S. Rakhia1, Ahmed Mohamed Khamis1
 ORCID
ORCIDRecibido: 08-10-2022
Aceptado: 14-12-2022
©2023 El(los) Autor(es) – Esta publicación es Órgano oficial de la Sociedad de Anestesiología de Chile
Revista Chilena de Anestesia Vol. 52 Núm. 4 pp. 374-379|https://doi.org/10.25237/revchilanestv52n04-08
PDF|ePub|RIS
Abstract
Background: The most used psychoactive substance worldwide is caffeine. Acute caffeine administration in a laboratory setting or caffeine as an adjuvant have been shown to have pain-relieving effects. The possible effects of habitual dietary caffeine consumption on the use of intraoperative analgesics and pain perception, however, are far less well understood. Methods: Design: A prospective observational exploratory pilot study. Setting: Single university teaching hospital’s operating rooms. Patients: After institutional approval of the study design, 90 surgical patients – scheduled for laparoscopic surgery- were surveyed about their average daily caffeine consumption. They were then grouped to either: non consumers, low caffeine consumers and high caffeine consumers. Objectives: This pilot study aimed to explore the relationship between the amount of daily dietary caffeine consumption and intraoperative analgesic requirements. Results: In this study, no significant difference was found between the three study groups as regard intraoperative analgesic requirements, hemodynamics, recovery time, postoperative headache, and postoperative sedation level. However -although statistically insignificant- both caffeine consumers groups had higher intraoperative analgesic consumption. Additionally, higher consumer group had earlier request time of postoperative 1st rescue analgesia. Conclusión: Despite the limitations of any pilot study, our results suggest that habitual caffeine -whether in low or high consumers- had no significant effect on intraoperative analgesic requirements, when compared to non-consumers group. The data presented require careful consideration and promote the need for further studies with larger sample size as our study is an exploratory pilot study with small sample size.
Resumen
La sustancia psicoactiva más utilizada a nivel mundial es la cafeína. Se ha demostrado que la administración aguda de cafeína en un entorno de laboratorio o la cafeína como adyuvante tiene efectos analgésicos. Sin embargo, los posibles efectos del consumo habitual de cafeína en la dieta sobre el uso de analgésicos intraoperatorios y la percepción del dolor son mucho menos conocidos. Métodos: Diseño: Estudio piloto prospectivo observacional exploratorio. Lugar: Quirófanos de un hospital docente universitario único. Pacientes: Después de la aprobación institucional del diseño del estudio, se encuestó a 90 pacientes quirúrgicos, programados para cirugía laparoscópica, sobre su consumo promedio diario de cafeína. Luego se agruparon en: no consumidores, consumidores bajos de cafeína y consumidores altos de cafeína. Objetivos: Este estudio piloto tuvo como objetivo explorar la relación entre la cantidad de consumo diario de cafeína en la dieta y los requisitos analgésicos intraoperatorios. Resultados: En este estudio no se encontró diferencia significativa entre los tres grupos de estudio en cuanto a los requerimientos analgésicos intraoperatorios, hemodinámica, tiempo de recuperación, cefalea posoperatoria y nivel de sedación posoperatoria. Sin embargo, aunque estadísticamente insignificante, ambos grupos de consumidores de cafeína tuvieron un mayor consumo de analgésicos intraoperatorios. Además, el grupo de consumidores más alto solicitó antes la primera analgesia de rescate posoperatoria. Conclusión: A pesar de las limitaciones de cualquier estudio piloto, nuestros resultados sugieren que la cafeína habitual, ya sea en consumidores bajos o altos, no tuvo un efecto significativo sobre los requerimientos analgésicos intraoperatorios, en comparación con el grupo de no consumidores. Los datos presentados requieren una cuidadosa consideración y promueven la necesidad de estudios adicionales con mayor.
-
Introduction
Approximately 90% of all adults in the world consume caffeine in their daily diet. In 2015, the European Food Safety Authority (EFSA) suggested that up to a daily 200 mg from all caffeine sources do not raise safety concerns[1]. Caffeine and adenosine are structurally similar, which allows caffeine to bind to adenosine receptors, block adenosine, and inhibit its effects. Adenosine is known to inhibit arousal and increase drowsiness, as it is an inhibitor of neuronal activity in the peripheral and central nervous systems. In moderate doses, caffeine can antagonize the effects of adenosine and reduce fatigue and increase alertness[2]. Additionally, caffeine shows pain relieving properties by blocking peripheral adenosine receptors on sensory afferents. Because of this, it has been included in many over the counter and prescription drugs[3]. Despite these effects, caffeine at dietary levels is not usually regarded as an analgesic on its own with very few available clinical data.
Given the forementioned data, we hypothesized that di- etary caffeine consumption would have favorable effects on perioperative analgesic consumption in laparoscopic surgeries with expected further decrease in analgesic needs in “high caffeine consumers” group. This study aimed to investigate the relationship between the amount of daily dietary caffeine consumption and intraoperative analgesic requirements.
-
Materials and Methods
-
Ethics
Ethical approval for this study (FMASU R 67/ 2022) was provided by the Ethics committee of university hospital on 19/4/2022. It also was registered at Clinical Trial Registry ClinicalTrials.gov Identifier: NCT05330754. Written informed con- sent was obtained from all applicants.
-
Inclusion criteria
We enrolled ninety patients who were: 18 – 65 years old, physical status American Society of Anesthesiology (ASA) I&II, scheduled to undergo elective laparoscopic surgery.
-
Exclusion criteria
Patients converted to an open surgery, and those with: psychological or nervous system diseases, uncontrolled cardiac ar- rhythmias, addicts, or smokers.
-
Patients’ recruitment
Preanesthetic check-up was done. Average daily caffeine consumption in mg was calculated according to “caffeine con- tent in consumed drinks” as estimated by “Food Data Central”[2],[4]. Products asked upon in the preanesthetic checkup were: regular/green coffee, instant coffee, espresso, decaffeinated coffee, black tea, green tea, cola drinks, energy beverages, dark chocolate, milk chocolate, and medication with caffeine. And accordingly, patients were grouped to one of 3 groups: 1. Control group: No caffeine intake.
2. Low caffeine consumers (Safe level) group: Caffeine daily intake < 200 mg/day.
3. High caffeine consumers (Unsafe level group): Caffeine daily intake > 200 mg/day.
The proposed classification is according to previous guide- lines[1].
-
Anesthesia and surgical procedure
Pre-oxygenation with 100% oxygen was done. General anesthesia was induced intravenously with propofol 2 mg/kg, fentanyl 1.5 pg/kg, and atracurium 0.5 mg/kg to be followed by orotracheal intubation after 3 minutes of manual ventilation. After securing of endotracheal tube, all patients were positioned to start the surgery and the laparoscopic procedure was carried out in a standard fashion. 1%-2% (vaporizer set- ting) of isoflurane mixed with oxygen (50%) and air (50%) was used for maintenance of anesthesia. Increments of 10 mg of atracurium were administered repetitively every 20 minutes to achieve muscle relaxation. Minute ventilation volume was adjusted to keep end tidal PCO2 at 35 mm Hg to 40 mm Hg. Mean arterial blood pressure (MABP) and heart rate (HR) were measured at specific time points. MABP rise of > 20% above baseline was treated by administering a 0.5 pg/kg intravenous bolus of fentanyl. At the end of surgery and after closure of skin incision, residual neuromuscular blockade was reversed and extubation was done. The time of arrival in the postoperative unit is defined as 0 h postoperatively. A fixed dose of intravenous paracetamol 1 gm was given every 6 hours to all patients in both groups starting from 0 h in PACU.
-
Patient reported outcomes
The primary outcome was “total intraoperative fentanyl consumption in microgram”. (Induction dose was not included).
Secondary aims:
1. Recovery time in minutes (time interval between discontinuation of isoflurane and extubation).
2. Intraoperative hemodynamics: MABP and HR were recorded at the following timings: preoperatively as baseline, after intubation, after abdominal insufflation, then every 15 minutes till end of surgery, and then every hour for 2 hours in PACU.
3. Timing of 1st rescue analgesia (5 mg Nalbuphine).
4. Assessment of postoperative sedation level using “University of Michigan Sedation Scale (UMSS)”[5]. It was assessed every hour for 2 hours starting from extubation.
Sample size
As this trial is considered a pilot study, and given the lack of clarity on the ideal sample size due to lack of related information on the relationship between habitual dietary caffeine consumption and perioperative analgesic requirements; a sample size of at least 30 cases per group was considered appropriate.
-
Statistical analysis
The collected data was revised, coded, tabulated and introduced to a PC using Statistical package for Social Science (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.) Shapiro wilk’s test was used to evaluate normal distribution of continuous data. Quantitative variables are expressed as mean and SD. Qualitative variables are expressed as frequencies and percent. ANOVA test was used to compare Quantitative variables between the three study groups. Post Hoc Test was used for comparisons of all possible pairs of group means. Chi square and Fisher’s exact test were used to examine the relationship between Categorical variables. Correlation analysis using Pearson/spearman’s method was used to assess the strength of association between two quantitative variables according to data distribution. A P- value< 0.05 was considered statistically significant.
-
Results
As regard personal data, there was no significant difference between the three study groups as regard age, gender, body mass index (BMI), sleeping hours and ASA-PS. Similarly, there was no significant difference between the three study groups as regard type of operation, duration of operation and recovery time (Table 1). As regard MABP and HR at baseline and at different follow up, no significant difference was found between the three study groups (Figure 1) (Figure 2). As regard analgesia, sedation and postoperative headache, no significant difference was found between the three study groups as regard total intraoperative fentanyl, timing of 1st rescue analgesia, sedation score and post-operative headache (Table 2). There was no significant correlation between average total caffeine consumption per day and each of total intraoperative fentanyl, timing of 1st rescue analgesia, and postoperative sedation sore (Table 3).
Table 1. Comparison between three groups as regard personal and medical characteristics
| Control | Group Low consumers
Mean ± SD | High consumers | P | Sig | |||
| Mean | ± SD | ||||||
| Mean | ± SD | ||||||
| Age (years) | 41.77 | 10.70 | 43.87 12.18 | 39.50 | 11.28 | 0.337* | NS |
| BMI | 35.30 | 8.05 | 35.25 8.31 | 37.13 | 9.45 | 0.631* | NS |
| Sleeping hours/day | 7.57 | 1.07 | 7.30 .84 | 7.23 | 1.10 | 0.406* | NS |
| Duration of operation (minutes) | 95.00 | 19.43 | 91.50 20.39 | 93.00 | 18.22 | 0.782* | NS |
| Recovery time (minutes) | 8.67 | 3.92 | 9.17 3.49 | 9.50 | 3.79 | 0.687* | NS |
| Gender Male | 11 | 36.7% | 11.00 36.70 | 12 | 40.0% | 0.954* | NS |
| Female | 19 | 63.3% | 19.00 63.30 | 18 | 60.0% | ||
| ASA-PS
ASA 1 | 19 | 63.3% | 18.00 60.00 | 22 | 73.3% | 0.527* | NS |
| ASA 2 | 11 | 36.7% | 12.00 40.00 | 8 | 26.7% | ||
| Laparoscopy
Cholecystectomy | 23 | 76.7% | 23.00 76.70 | 20 | 66.7% | 0.77** | NS |
| Colostomy | 1 | 3.3% | 2.00 6.70 | 0 | 0.0% | ||
| Gastric bypass | 2 | 6.7% | 1.00 3.30 | 3 | 10.0% | ||
| Hernia repair | 2 | 6.7% | 2.00 6.70 | 2 | 6.7% | ||
| Gastrectomy | 2 | 6.7% | 2.00 6.70 | 5 | 16.7% | ||
*ANOVA test.
*Chi-Square Tests.
**Fisher exact test.
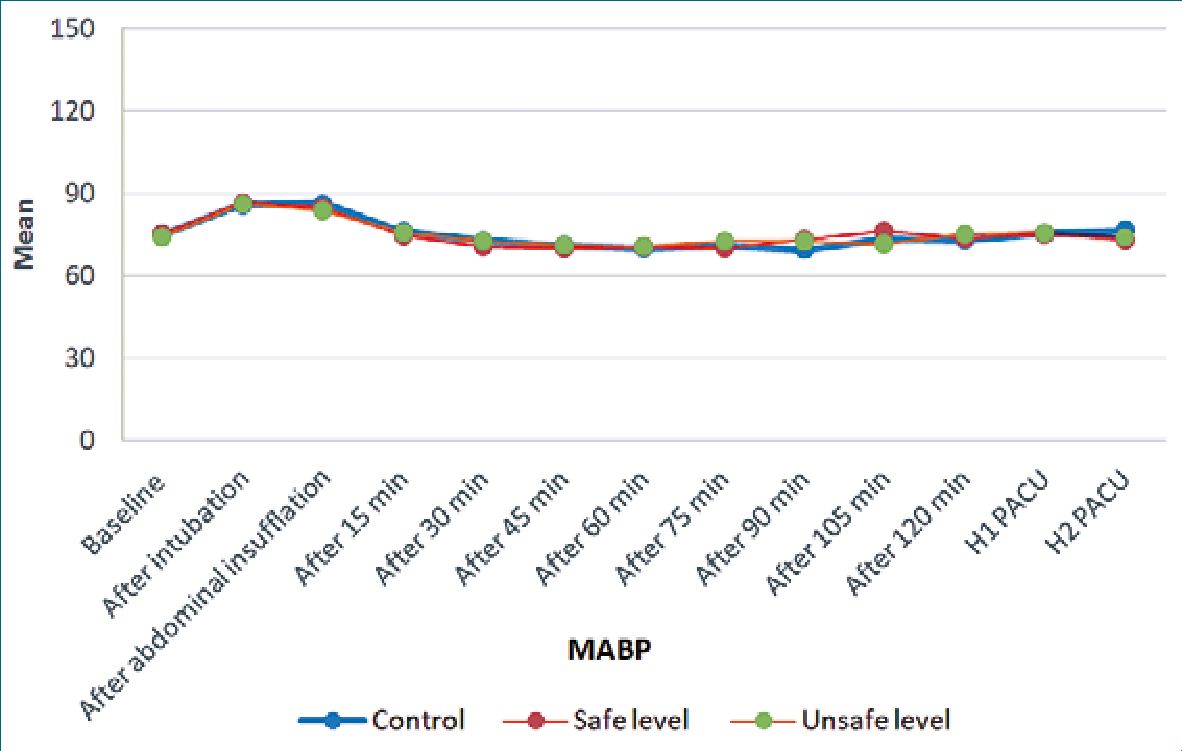
Figure 1. Comparison between three groups as regard MABP.
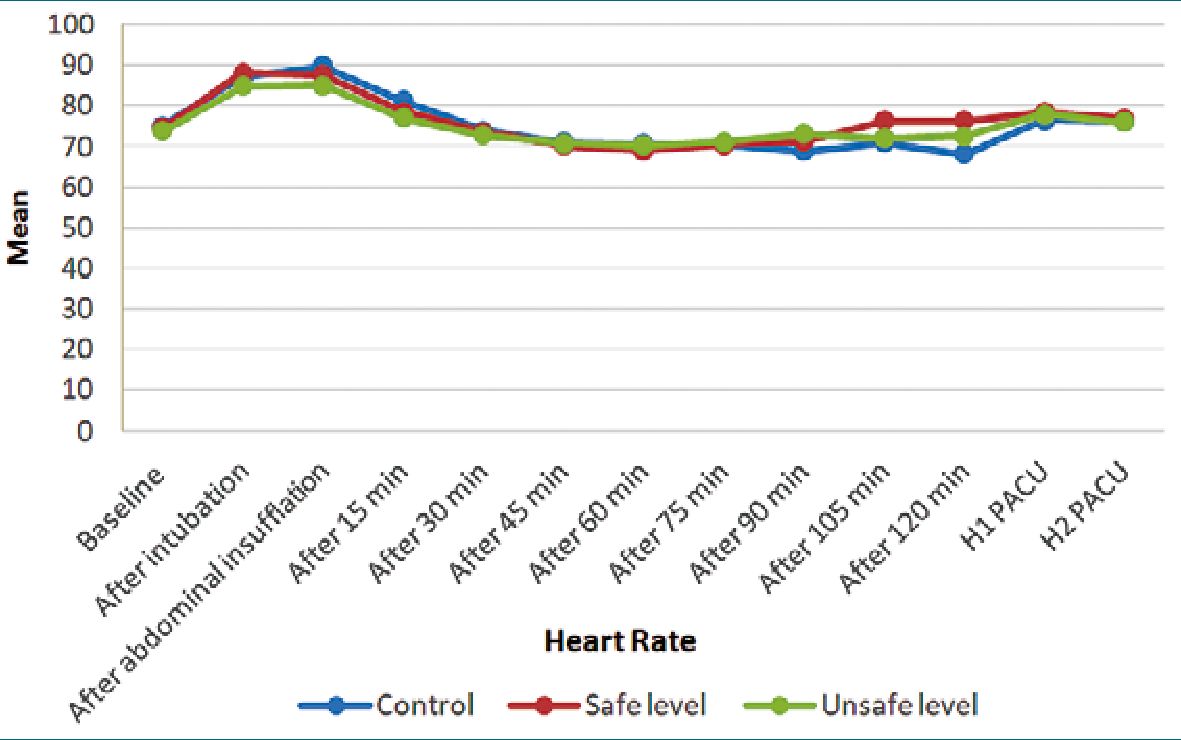
Figure 2. Comparison between three groups as regard HR.
-
Discussion
Caffeine administered acutely in a laboratory environment or as a medication adjuvant has known properties that help alleviate pain. Consistent evidence showed that antagonism of adenosine receptors by caffeine leads to decreased pain signaling in animal models for neuropathic, nociceptive, and inflammatory pain[6]. However, much less is known about the potential impact of habitual dietary caffeine consumption in relation to clinical pain alleviation. Exploratory pilot research is a methodology approach that explores research questions that have not previously been studied in depth. It is often used when the issue to be studied is new. In this exploratory pilot study, our observed results didn’t support our expectation in confirming dietary caffeine analgesic potential. But since it is an exploratory pilot study, it could be beneficially considered as a hypothesis generating study that could be utilized by future studies with larger sample size.
We observed that habitual caffeine -whether in low or high consumers- has no effect on intraoperative analgesic requirements, when compared to non-consumers group. We might contribute this observation to the following: 1- the development of caffeine tolerance due to habitual consumption might impacts pain sensitivity through the upregulation of adenosine receptors[7]. 2- The effects of caffeine usually last from 8 to 12 hours[2]. But since surgical patients are often instructed to fast; they are at risk for experiencing fading of caffeine’s effects (whether analgesic or stimulatory effects). 3- variable effect of caffeine on analgesic pathway8. The nociceptive effects of caffeine are associated with its nonselective antagonism of the adenosine A1, A2A, A2B and A3 receptor[3]. Adenosine has a dual nature in that it is a molecule that can cause and relieve pain via different adenosine receptors. Adenosine acts as an analgesic when acting through A1 receptors, which are central receptors, adenosine also contributes to chronic pain through its A2b receptors, which are peripheral receptors. This means that, caffeine’s analgesic effect depends on which adenosine receptor was more blocked[8].
Noteworthy, although statistically insignificant, non-consumers group had marginal less intraoperative fentanyl requirements when compared to either low or high consumers groups (170 ± 34 pg in non-consumers group, versus 178 ± 31 pg & 180 ± 31 pg in low and high consumers groups respectively). Additionally, earlier request of 1st rescue analgesia was observed in caffeine high consumers’ group (83.50 ± 24 minutes in high consumers group, versus 90.33 ± 29 minutes & 92.41 ± 35 minutes in control and low consumers groups respectively). But it was also statistically insignificant. Since the current research protocol required subjects to fast for 8 hours preoperatively, it is likely that some subjects experienced caffeine withdrawal. Due to this acute abstinence of caffeine consumption, it is conceivable that some subjects may have been experiencing “caffeine withdrawal increased pain sensitization”, which could be reflected in either higher intraoperative fentanyl consumption or earlier request of postoperative 1st rescue analgesia.
Table 2. Comparison between three groups as regard analgesia, sedation and postoperative headache
| Group | P | Sig | ||||||
| Control | Low consumers | High consumers | ||||||
| Mean | ± SD | Mean | ± SD | Mean | ± SD | |||
| Total intraoperative Fentanyl (microgram) | 170.00 | 33.73 | 178.33 | 31.30 | 180.00 | 31.07 | 0.436* | NS |
| Timing of 1 st rescue (minutes) | 90.33 | 28.74 | 92.41 | 35.45 | 83.50 | 23.53 | 0.481* | NS |
| UMSS H, 0 | 11 | 36.7% | 16 | 53.3% | 14 | 46.7% | 0.709** | NS |
| 1 | 18 | 60.0% | 13 | 43.3% | 14 | 46.7% | ||
| 2 | 1 | 3.3% | 1 | 3.3% | 2 | 6.7% | ||
| UMSS H2 0 | 30 | 100.0% | 30 | 100.0% | 29 | 96.7% | 1.00** | NS |
| 1 | 0 | 0.0% | 0 | 0.0% | 1 | 3.3% | ||
| PO headache
No | 26 | 86.7% | 25 | 83.3% | 25 | 83.3% | 1.00** | NS |
| Yes | 4 | 13.3% | 5 | 16.7% | 5 | 16.7% | ||
*ANOVA test.
**Fisher exact test.
Table 3. Correlation between average total Caffeine consumption per day in mg and analgesic and sedation parameters
| Total intraoperative Fentanyl | Timing of 1st rescue | UMSS H1 | UMSS H2 | |
| Average consumption Correlation coefficient | 0.160* | -0.169* | 0.141** | 0.109** |
| P | 0.223 | 0.201 | 0.281 | 0.407 |
| sig | NS | NS | NS | NS |
*Pearson correlation.
**Spearman correlation.
Antagonizing our results, previous studies[7],[9] showed that individuals who habitually consume greater amounts of caffeine as part of their daily diets demonstrate diminished sensitivity to painful stimuli in a laboratory setting. The results were the same whether subjects were abstaining caffeine before the procedure[9] or not[7]. These studies suggested that high dietary caffeine consumption may be sufficient to alter the nociceptive processing of pain signals in ways that significantly decrease sensitivity to painful stimuli. On the other hand, Alobaid and their colleagues[10], showed increased failure rates and delayed onset of local anesthetic among high caffeine consumers in fasting female patients undergoing dental procedure. This high failure rate could be attributed to caffeine’s influence on cognitive performance by increasing alertness and augmented response to painful stimuli, as well as sleep deprivation caused by stress and anxiety[8]. Another interesting study by Karunathilake and their colleagues[11], performed baseline experimental pain testing and caffeine plasma concentrations (CPC) sampling on 30 healthy adults before and after surgical extraction of four third molars. Their study found that baseline pain sensitivity was higher among individuals who self-reported positive caffeine consumption. But on the other hand, caffeine seemed to have an antinociceptive effect postoperatively in individuals with CPC > 300 ng/mL.
Finally, surgical patients routinely fast preoperatively and may have postoperative symptoms from caffeine withdrawal. While there are several well-defined symptoms of caffeine withdrawal syndrome, the literature has focused on headache as the primary endpoint of assessing, preventing, and treating caffeine withdrawal. The onset of withdrawal symptoms typically occurs 12-24 hours after caffeine last intake but can occur as early as 3-6 hours post-ingestion especially in high consumers[12]. Unfortunately, this headache may be easily ascribed to other causes, masking the recognition of caffeine withdrawal as the causative source. In our study, postoperative headache symptom was not significant between the 3 groups. This could be attributed to variable causes of postoperative headache after general anesthesia which could mask the real prevalence of caffeine withdrawal headache.
Our study is not without limitation. Firstly, and most importantly, this is an exploratory pilot study. This means that our sample size might be too small to detect significant changes in the evaluated outcomes between the 3 groups. A sample size of at least 90 patients per group is recommended. Secondly, measurement error can affect the assessment of caffeine intake. As some beverages asked upon in the preanesthetic checkup were not brand or type specific. Additionally, coffee bean type, and the quantity of milk or cream added to coffee are typically not recorded. As a result, caffeine cannot be accurately quantified, and more research are needed with larger sample size and more accurate caffeine estimation in order to draw more obvious conclusions. Finally, preoperative chronic pain, analgesics, and anxiety disorders that affect perioperative pain was not recorded.
-
Conclusion
Despite the limitations of a pilot study, our results suggest that habitual caffeine -whether in low or high consumers- had no significant effect on intraoperative analgesic requirements, when compared to non-consumers group. The data presented require careful consideration and promote the need for further studies with larger sample size as it is an exploratory pilot study with small sample size.
Assistance with the article: None.
Financial support and sponsorship: None.
Conflicts of interest: None.
Presentation: None.
Trial Registration: NCT05330754
References
1. El-Nimr NA, Bassiouny SH, Tayel DI. Pattern of caffeine consumption among university students. JHIPH. 2019 Dec;49(3):154–61. https://doi.org/10.21608/jhiph.2019.56579.
2. van Dam RM, Hu FB, Willett WC. Coffee, caffeine, and health. N Engl J Med. 2020 Jul;383(4):369–78. https://doi.org/10.1056/NEJMra1816604 PMID:32706535
3. Piekarska E, Pawlicki M, Łopuszynska A, Kozioł M, Krasa A, Piecewicz-Szczesna H. Caffeine in Pain Perception and Management. J Educ Health Sport. 2021 Aug;11(8):328–33. https://doi.org/10.12775/JEHS.2021.11.08.036.
4. Mitchell DC, Knight CA, Hockenberry J, Teplansky R, Hartman TJ. Beverage caffeine intakes in the U.S. Food Chem Toxicol. 2014 Jan;63:136–42. https://doi.org/10.1016/j.fct.2013.10.042 PMID:24189158
5. Malviya S, Voepel-Lewis T, Tait AR, Merkel S, Tremper K, Naughton N. Depth of sedation in children undergoing computed tomography: validity and reliability of the University of Michigan Sedation Scale (UMSS). Br J Anaesth. 2002 Feb;88(2):241–5. https://doi.org/10.1093/bja/88.2.241 PMID:11878656
6. Sawynok J. Adenosine receptor targets for pain. Neuroscience. 2016 Dec;338:1–18. https://doi.org/10.1016/j.neuroscience.2015.10.031 PMID:26500181
7. Overstreet DS, Penn TM, Cable ST, Aroke EN, Goodin BR. Higher habitual dietary caffeine consumption is related to lower experimental pain sensitivity in a community-based sample. Psychopharmacology (Berl). 2018 Nov;235(11):3167–76. https://doi.org/10.1007/s00213-018-5016-3 PMID:30187108
8. Premnath S, Alalshaikh G, Alfotawi R, Philip M. The association between coffee consumption and local anesthesia failure: social beliefs and scientific evidence. Cureus. 2020 Apr;12(4):e7820. https://doi.org/10.7759/cureus.7820 PMID:32467795
9. Haskell-Ramsay CF, Jackson PA, Forster JS, Dodd FL, Bowerbank SL, Kennedy DO. The acute effects of caffeinated black coffee on cognition and mood in healthy young and older adults. Nutrients. 2018 Sep;10(10):1386. https://doi.org/10.3390/nu10101386 PMID:30274327
10. Alobaid AS, Hussain OA, Alamoudi NA, Alshahrani YA, Almuaddi AF, Almathami AA. Effect of caffeine on the onset, efficiency and duration of local anaesthesia among female patients. An original research. Int J Med Dent. 2019 Jan;23:138–44.
11. Karunathilake NP, Frye RF, Stavropoulos MF, Herman MA, Hastie BA. A preliminary study on the effects of self-reported dietary caffeine on pain experience and postoperative analgesia. J Caffeine Res. 2012 Dec;2(4):159–66. https://doi.org/10.1089/jcr.2012.0016 PMID:24761271
12. Agritelley MS, Goldberger JJ. Caffeine supplementation in the hospital: potential role for the treatment of caffeine withdrawal. Food Chem Toxicol. 2021 Jul;153:112228. https://doi.org/10.1016/j.fct.2021.112228 PMID:33932520