
Gianpaolo Cecioni Pineda1, Xue Zou2
 ORCID
ORCID
Recibido: 2025-10-27
Aceptado: 2026-01-15
©2026 El(los) Autor(es) – Esta publicación es Órgano oficial de la Sociedad de Anestesiología de Chile
Revista Chilena de Anestesia Vol. 55 Núm. 3 | https://doi.org/10.25237/revchilanestv55n3-18
PDF
Consideraciones anestésicas en la nefrectomía radical bilateral en un paciente de 11 meses: Reporte de caso
Abstract
We report the anesthetic management of an 11-month-old infant diagnosed with a suspected bilateral Wilms tumor (stage V), associated with a germline WT1 mutation and refractory to first-line chemotherapy (AREN0534 protocol). Due to lack of response, treatment was shifted to the Umbrella SIOP 2016 protocol. The patient also had a history of hypertension, proteinuria, and bilateral cryptorchidism. A radical bilateral nephrectomy and right adrenalectomy were performed. The procedure was complicated by inadvertent sectioning of the inferior vena cava (IVC), requiring vascular reconstruction and subsequent therapeutic anticoagulation due to a distal thrombus. Anesthesia was managed with particular attention to rapid sequence induction, intraoperative hemodynamic stability, perioperative bleeding risk, postoperative pain control, and renal failure requiring dialysis. This case highlights four key anesthetic considerations: 1) preparation for rapid sequence induction; 2) anticipation of hemodynamic instability and bleeding complications; 3) management of epidural analgesia in the context of unexpected anticoagulation, and 4) perioperative planning for anticipated dialysis. This report highlights principles applicable to any high-risk pediatric surgery: anticipate complications, adapt rapidly, and always prioritize neurologic and hemodynamic safety in the anesthetic plan.
Resumen
We report the anesthetic management of an 11-month-old infant diagnosed with a suspected bilateral Wilms tumor (stage V), associated with a germline WT1 mutation and refractory to first-line chemotherapy (AREN0534 protocol). Due to lack of response, treatment was shifted to the Umbrella SIOP 2016 protocol. The patient also had a history of hypertension, proteinuria, and bilateral cryptorchidism. A radical bilateral nephrectomy and right adrenalectomy were performed. The procedure was complicated by inadvertent sectioning of the inferior vena cava (IVC), requiring vascular reconstruction and subsequent therapeutic anticoagulation due to a distal thrombus. Anesthesia was managed with particular attention to rapid sequence induction, intraoperative hemodynamic stability, perioperative bleeding risk, postoperative pain control, and renal failure requiring dialysis. This case highlights four key anesthetic considerations: 1) preparation for rapid sequence induction; 2) anticipation of hemodynamic instability and bleeding complications; 3) management of epidural analgesia in the context of unexpected anticoagulation, and 4) perioperative planning for anticipated dialysis. This report highlights principles applicable to any high-risk pediatric surgery: anticipate complications, adapt rapidly, and always prioritize neurologic and hemodynamic safety in the anesthetic plan.
Introduction
Wilms tumor represents the most prevalent kidney cancer in the pediatric population. It occurs with an incidence of approximately 9.7 per million children under the age of 15, increasing to 13.5 per million in infants[1]. Management involves a multimodal approach combining chemotherapy, surgical resection, and, when necessary, renal replacement therapy. From an anesthetic standpoint, these cases pose significant challenges, particularly in infants, due to physiological immaturity, organ dysfunction, coagulopathies, anemia, and sudden hemodynamic shift[2].
In the present case, we describe the anesthetic management of an 11-month-old infant undergoing radical bilateral nephrectomy and right adrenalectomy following chemotherapy failure. The procedure was complicated by accidental inferior vena cava (IVC) injury, requiring vascular reconstruction and therapeutic anticoagulation. Anesthetic planning included rapid sequence induction, preparedness for hemorrhagic shock, cautious use of epidural analgesia with anticipated early removal, and coordination for postoperative dialysis. This report highlights the key anesthetic considerations relevant to highrisk pediatric oncologic surgery.
Case presentation
An 11-month-old male infant, weighing 11.5 kg, with a bilateral Wilms tumor (stage V), germline WT1 mutation, and no response to initial chemotherapy (AREN0534 protocol), was scheduled for radical bilateral nephrectomy with initial plan for bilateral adrenalectomy. His past medical history included hypertension on amlodipine (secondary to oncologic medication), bilateral cryptorchidism, proteinuria, and a resolved thrombocytopenia secondary to chemotherapy. The chemotherapy protocol had recently been modified to the Umbrella SIOP 2016 regimen (etoposide, carboplatin) due to poor response. Preoperative imaging showed progressive enlargement of both renal masses, with mass effect on the inferior vena cava (IVC), but no overt signs of invasion. Echocardiography was normal. A CT scan revealed right and left renal masses measuring 13.8×10.8×16.2 cm and 11.2×8.9×14.1 cm, respectively, both with necrotic components (Figure 1). There was a visible mass effect on the IVC and an enlarged azygos vein, suggesting collateral circulation. Clinically, the patient needed to be in a semi-upright position with 0.5 L/min of supplemental oxygen to maintain saturations > 95%, as the bilateral renal masses compressed the diaphragm and lower lung fields, causing basal atelectasis. No neurological deficit was present. The patient was admitted for surgical management with a two-phase procedure.
In the first phase, the patient was taken to the interventional radiology suite for placement of a tunneled peritoneal dialysis catheter. He arrived with nasal cannula oxygen at 0.5 L/min. A rapid sequence induction (RSI) was performed with the patient maintained in his semi-upright position using midazolam, ketamine, sufentanil, and rocuronium, using an existing upper extremity PICC line. Orotracheal intubation was successful on the first attempt (Cormack-Lehane grade 1). Desaturation occurred easily but resolved, and the patient remained hemodynamically stable without vasopressor support. General anesthesia was maintained with inhaled agents during this portion. The dialysis catheter was inserted uneventfully. The patient was then transferred, intubated and sedated, to the operating room.
The second phase took place in the operating room, anesthesia was transitioned to intravenous agents, including ketamine, dexmedetomidine, and sufentanil. A 22G peripheral IV was placed on the right, and a 22G radial arterial line was inserted in the left wrist. The patient was positioned in left lateral decubitus for epidural catheter placement under sterile conditions (Touhy 18G needle, 20G catheter). The epidural catheter was placed on the first attempt under clean technique, with no blood or cerebrospinal fluid observed, a test dose of 3 mL bupivacaine 0.1% with epinephrine 1:200,000 was administered and showed no evidence of intrathecal or intravascular place ment. Surgical access was gained via midline laparotomy. Intraoperative monitoring of anesthetic depth was utilized; however, given the patient’s age, BIS values were considered less reliable[3]. Therefore, interpretation focused primarily on DSA patterns and SEF95, confirming an adequate depth of anesthesia. Fluid management consisted of lactated Ringer’s solution and 5% albumin, guided by serial laboratory testing. During the right renal tumor excision, the inferior vena cava was accidentally transected, necessitating vascular reconstruction and eventual therapeutic anticoagulation. Upon identification of the IVC injury and the need for vascular reconstruction and use of systemic anticoagulation, the surgical team promptly informed the anesthesiologist. Aware of the epidural catheter, a brief multidisciplinary discussion ensued. Although the catheter had been atraumatically placed, it was preemptively removed to minimize the risk of epidural hematoma. Intravenous heparin (10 IU/kg/h) was initiated one hour later. Total IVC clamping time was 22 minutes. The left tumor resection proceeded uneventfully (Figure 2).
Intraoperative ultrasound revealed a distal thrombus in the IVC. A 100 IU/kg heparin bolus was administered, followed by Fogarty catheter thrombectomy, with restoration of satisfactory flow confirmed on repeat imaging.
The patient received 450 mL of packed red blood cells. He required brief support with norepinephrine (maximum 0.07 mcg/kg/min) and epinephrine (maximum 0.05 mcg/kg/min), both weaned prior to closure. He was transferred intubated to the pediatric intensive care unit (PICU).

Figure 1. Coronal CT scan of the abdomen demonstrating bilateral renal masses in an 11-month-old infant. Large, well-circumscribed masses are visualized in both renal fossae, consistent with bilateral Wilms tumors. The tumors cause significant mass effect, displacing intra-abdominal organs and compressing adjacent structures. The left tumor appears to compress the liver superiorly, while the right tumor shifts the midline and abuts the diaphragm.
In the PICU, the patient remained intubated and sedated postoperatively. Extubation was performed the following morning without complication. Initial laboratory workup showed a metabolic acidosis (bicarbonate 15 mmol/L), stable potassium (3.6 mmol/L), and no immediate indication for dialysis. However, persistent acidosis and rising uremia led to the initiation of hemodialysis on postoperative day two. Anticoagulation was maintained with intravenous heparin at 23 IU/kg/h, adjusted according to anti-Xa levels. Imaging confirmed a residual non-obstructive thrombus in the IVC. Other complications included mild right-sided pleural effusion and postoperative ileus managed conservatively with nasogastric suction. Hydro
cortisone was discontinued on postoperative day three, with planned cortisol monitoring to evaluate for potential adrenal insufficiency.
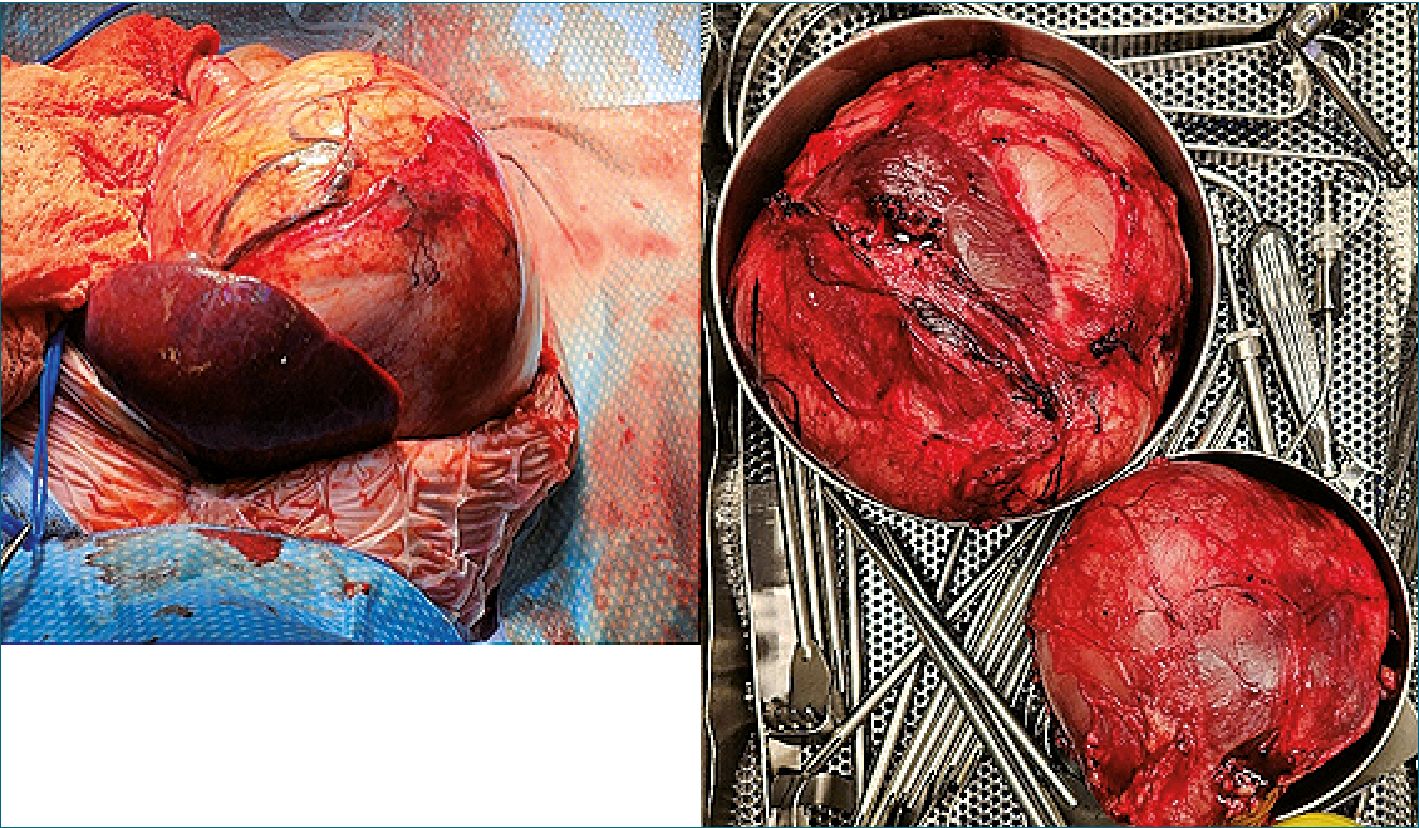
Figure 2. (Left): Intraoperative view of the right-sided tumor occupying most of the abdominal cavity, displacing adjacent organs. The liver is seen anteriorly, partially covering the tumor surface. (Right): Gross appearance of both resected renal tumors following radical bilateral nephrectomy. The tumors exhibit well-encapsulated, lobulated masses with prominent vascularization.
Discussion
1. Airway Management and Induction Strategy
Airway management in infants undergoing major abdominal surgery requires precise planning due to anatomical and physiological characteristics such as a proportionally larger tongue, cephalad larynx, high metabolic rate, and limited oxygen reserve[4]. In this case, the patient had large bilateral abdominal tumors causing mass effect and increased intra-abdominal pressure, which elevated the risk of aspiration, thereby justifying RSI despite the non-emergency setting.
The induction was carried out in a semi-upright position, to optimize preoxygenation and preserve diaphragmatic excursion. A combination of midazolam, ketamine, sufentanil, and rocuronium was used to achieve rapid hypnosis, analgesia, neuromuscular blockade, and cardiovascular stability. Intubation was successful on the first attempt. Despite adequate preoxygenation, rapid desaturation occurred, a common phenomenon in this age group due to high oxygen consumption and low functional residual capacity[5]. In this case, the presence of large abdominal masses further compromised respiratory mechanics by exerting pressure on the lungs, leading to basal atelectasis and an further reduction in functional residual capacity.
2. Hemodynamic preparation and anticipation of bleeding
Given the anticipated surgical complexity and potential for major blood loss, meticulous hemodynamic preparation was essential. The patient arrived in the angiography suite with a pre-existing peripherally inserted central catheter (PICC), which allowed for a controlled intravenous induction with better hemodynamic stability rather than an inhalational approach[6].
Although the tunneled dialysis catheter was placed primarily for potential postoperative renal replacement therapy, it also served as an emergency venous access for volume resuscitation, if needed. A new 22-gauge peripheral intravenous line was added in the right hand, providing additional access appropriate for fluid administration in a child of this size.
The PICC was used for the administration of vasoactive agents and hypnotic drugs, with preloaded epinephrine and norepinephrine syringes connected and ready at induction. This ensured immediate availability of inotropes in case of hemodynamic instability. A left radial arterial catheter was inserted to enable continuous blood pressure monitoring, waveform assessment, and repeated arterial blood sampling. This allowed for timely detection of changes in perfusion status and guided transfusion decisions throughout the procedure.
Fluid and blood product preparation included: Ringer’s lactate, 5% albumin for volume support, and crossmatched packed red blood cells. Laboratory follow-up was done intraoperatively to monitor hemoglobin, coagulation status, and acid-base balance, ensuring appropriate timing of interventions.
This multi-access vascular strategy, along with ready-to-use vasoactive drugs and transfusion resources, reflects current best practice in high-risk pediatric surgery[7]. Anticipating blood loss and preparing for real-time hemodynamic shifts are essential for reducing morbidity in major tumor resections involving large abdominal masses and major vessels.
- Postoperative pain management and epidural catheter removal
Epidural analgesia remains a cornerstone of multimodal pain management in pediatric major abdominal surgery, offering superior analgesia compared to systemic opioids and potentially reducing postoperative complications. However, neuraxial hematoma, although rare, is a serious complication associated with the epidural technique, most commonly occurring during or after catheter removal, and may result in devastating neurological outcomes.
Current guidelines discourage the continued use of neurax- ial or deep plexus catheters in patients receiving continuous intravenous heparin infusions. If postoperative anticoagulation becomes unexpectedly necessary, strict neurological monitoring is imperative. In such cases, employing the lowest effective concentration of local anesthetics is crucial to allow prompt detection of any neurological deficits[8].
For pediatric patients in particular, timely removal of the epidural catheter prior to initiating therapeutic anticoagulation is critical. The consequences of an epidural hematoma can be catastrophic, and detection is further complicated by age-related limitations in verbal communication and subtle presentation of neurological symptoms. The American Society of Regional Anesthesia and Pain Medicine (ASRA) emphasizes precise timing between neuraxial procedures and the administration of anticoagulants to minimize the risk of spinal hematoma for- mation[8]. According to ASRA guidelines, a minimum interval of one hour is recommended between catheter removal and initiation of therapeutic unfractionated heparin, provided coagulation parameters are normal. This interval accounts for the pharmacodynamics of heparin and allows sufficient time for the needle tract to seal, reducing the likelihood of epidural bleeding[8].
In the present case, although the epidural catheter was placed atraumatically and remained complication-free, the dynamic and unpredictable nature of the patient’s anticoagulation requirements introduced a significant risk that could not be ignored. Delaying anticoagulation solely to preserve the epidural catheter was not a viable option given the urgent need for vascular repair and thrombus control. Had the catheter been retained, its eventual removal would have necessitated interruption of heparin therapy, normalization of coagulation indices (e.g., aPTT or anti-Xa), and a sustained anticoagulant free interval conditions that were neither practical nor safe in the context of active vascular pathology. Therefore, the decision to remove the epidural catheter prior to initiating anticoagulation was both consistent with published safety guidelines8 and clinically necessary. This approach prioritized neurological safety without compromising vascular management, illustrating the importance of individualized, risk-informed decision-making in anesthetic practice.
This case highlights the critical balance between optimizing analgesia and ensuring neurologic safety when urgent anticoagulation is required in pediatric patients with epidural catheters. Prompt interdisciplinary communication and adherence to safety standards were essential to prevent a potentially catastrophic complication.
- Postoperative preparation: dialysis and adrenal replacement therapy
Given the absence of preoperative renal function recovery and the tumor burden involving both kidneys, postoperative renal failure and dialysis were considered highly probable. The anesthetic plan included measures to facilitate early renal support while maintaining hemodynamic stability and minimizing nephrotoxic exposure.
A tunneled peritoneal dialysis catheter had been placed during the initial phase of the procedure, allowing for early initiation of renal replacement therapy if needed. This access proved critical, as by postoperative day 2, the patient developed persistent metabolic acidosis and rising uremic markers, prompting the start of dialysis.
In parallel, the initial surgical plan included bilateral adrenalectomy, which would have necessitated long-term corticosteroid replacement. Although residual adrenal tissue was unexpectedly preserved, this was only confirmed at the end of surgery. Given the patient’s exposure to chemotherapy and the anticipated adrenal suppression, perioperative stress-dose steroid therapy was administered preemptively. The patient received Solu-Cortef 50 mg IV at induction, followed by 12 mg IV every 6 hours, in accordance with pediatric adrenal insufficiency protocols[9],[10].
Fluid management was carefully tailored using crystalloids and 5% albumin, with close monitoring of urine output (with the expectation of post-nephrectomy anuria), acid-base status, lactate, and electrolytes. Red blood cell transfusions were available and administered as needed to maintain oxygen delivery without fluid overload.
Pain management was adjusted after epidural removal to avoid NSAIDs or agents with potential nephrotoxicity. Opioid use was titrated carefully based on the patient’s evolving renal clearance and neurological status.
Conclusion
This case highlights the complexity of anesthetic management in a high-risk infant undergoing radical bilateral nephrectomy. The presence of massive abdominal tumors, limited respiratory reserve, anticipated hemodynamic fluctuations, and the need for postoperative renal replacement therapy demanded meticulous planning. The use of rapid sequence induction, targeted vascular access, and multimodal monitoring ensured safe progression through both surgical stages. The intraoperative decision to remove the epidural catheter in anticipation of therapeutic anticoagulation exemplifies the dynamic, interdisciplinary collaboration required in pediatric anesthesia. Ultimately, balancing analgesic efficacy, neurologic safety, and evolving surgical priorities was key to achieving a favorable outcome in a medically fragile patient.
Referencias
1. National Cancer Institute: NCCR*Explorer: An interactive website for NCCR cancer statistics. Bethesda, MD: National Cancer Institute. Available online. Last accessed February 25, 2025.
2. Matinyan N, Saltanov A, Martynov L, Kazantsev A. Anesthesia management of a 20-month-old patient with giant unilateral wilms tumor. Case Rep Anesthesiol. 2015;2015:487219. https://doi.org/10.1155/2015/487219PMID: https://pubmed.ncbi.nlm.nih.gov/25815216
3. Grasso C, Marchesini V, Disma N. Applications and Limitations of Neuro-Monitoring in Paediatric Anaesthesia and Intravenous Anaesthesia: A Narrative Review. J Clin Med. 2021 Jun;10(12):2639. https://doi.org/10.3390/jcm10122639PMID: https://pubmed.ncbi.nlm.nih.gov/34203942
4. Disma N, Asai T, Cools E, Cronin A, Engelhardt T, Fiadjoe J, et al.; and airway guidelines groups of the European Society of Anaesthesiology and Intensive Care (ESAIC) and the British Journal of Anaesthesia (BJA). Airway management in neonates and infants: European Society of Anaesthesiology and Intensive Care and British Journal of Anaesthesia joint guidelines. Eur J Anaesthesiol. 2024 Jan;41(1):3–23. https://doi.org/10.1097/EJA.0000000000001928PMID: https://pubmed.ncbi.nlm.nih.gov/38018248
5. Choudhary, Annu; Singh, Swati; Kumar, Saurabh. Pediatric airway management: A narrative review of the current practices and challenges. Journal of Indira Gandhi Institute of Medical Sciences 10(2):p 100-106, Jul–Dec 2024. | https://doi.org/10.4103/jigims.jigims_19_24.
6. Swetha P, Surekha G, Rosanna S, Panati D. Comparison of intravenous vs. inhalational anesthetics in pediatric surgery: a cross-sectional analysis. J Chem Health Risks. 2025;15(2):844–8.
7. Lemson J, Nusmeier A, van der Hoeven JG. Advanced hemodynamic monitoring in critically ill children. Pediatrics. 2011 Sep;128(3):560–71. https://doi.org/10.1542/peds.2010-2920PMID: https://pubmed.ncbi.nlm.nih.gov/21824877
8. Kopp SL, Vandermeulen E, McBane RD, et al. Reg Anesth Pain Med, Epub ahead of print: 01-08-2025. https://doi.org/10.1136/rapm-2024-105766.
9. Heath C, Johnston A, Siafarikas A, Price G, von Ungern-Sternberg BS. Perioperative steroid prophylaxis for adrenal insufficiency, a single-centre experience. Paediatr Anaesth. 2024 Mar;34(3):274–6. https://doi.org/10.1111/pan.14797PMID: https://pubmed.ncbi.nlm.nih.gov/37947252
10. Bornstein SR, Allolio B, Arlt W, Barthel A, Don-Wauchope A, Hammer GD, et al. Diagnosis and Treatment of Primary Adrenal Insufficiency: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2016 Feb;101(2):364–89. https://doi.org/10.1210/jc.2015-1710PMID: https://pubmed.ncbi.nlm.nih.gov/26760044


